



Article reviewed by: Dr. Sturz Ciprian, Dr. Tîlvescu Cătălin and Dr. Alina Vasile
Article updated on: 22-06-2026
Mandibular osteoradionecrosis: what it is, how it develops, and how hyperbaric therapy helps
- What is mandibular osteoradionecrosis?
- Who is at risk of mandibular osteoradionecrosis?
- Symptoms of mandibular osteoradionecrosis and warning signs
- Why does the bone no longer heal by itself after radiotherapy?
- How does hyperbaric therapy (HBOT) help in mandibular osteoradionecrosis?
- The hyperbaric therapy protocol in osteoradionecrosis
- Total number of sessions and monitoring
- Prevention of mandibular osteoradionecrosis: how can this complication be avoided?
- Why does access to a specialized hyperbaric medical center matter?
There are medical complications that do not appear immediately, but settle in silently, months or even years after a treatment that, at the time, was meant to save your life. Mandibular osteoradionecrosis is one of them. It is a serious, often disabling condition that occurs in patients who have undergone radiotherapy for head and neck cancers. The mandibular bone, already weakened by irradiation, begins to die from the inside, without being able to regenerate on its own anymore.
What makes this complication even harder to manage is that there is no miraculous, fast, and completely effective treatment in every situation. Its treatment requires patience, multidisciplinarity, and a deep understanding of the biological mechanisms that led to this situation. Hyperbaric oxygen therapy (HBOT) has emerged in recent decades as one of the most valuable tools available to physicians who care for these patients, not as an alternative to surgery, but as its ally.
What is mandibular osteoradionecrosis?
To understand what osteoradionecrosis (abbreviated ORN) is, we must start from a simple fact: every living bone constantly needs blood. Bones are not static, inert structures; they renew themselves continuously through specialized cells that build and break down the bone matrix every day of life. If the blood supply is compromised, the bone stops functioning as living tissue and becomes, in essence, a necrotic fragment trapped inside the body.
Mandibular osteoradionecrosis is precisely this: the progressive death of the lower jaw bone as a direct consequence of radiotherapy applied to the head and neck area. The European Orphanet organization defines it as a condition characterized by exposure of irradiated bone that fails to heal over a period of at least three months, in the absence of any persistent or recurrent tumor. In other words, the bone is exposed, does not become covered, does not repair itself, and the process tends to worsen in the absence of intervention.
The mandible is the bone most frequently affected. According to an analysis published on PubMed Central, 95% of osteoradionecrosis cases in the head and neck area involve the mandible. The explanation is anatomical: the mandible is less vascularized than the upper jaw, has a thinner periosteum, and is constantly exposed to microtrauma through the simple action of chewing and speaking. Add to this the destructive effects of ionizing radiation on blood vessels and you obtain an extremely vulnerable bone.
The classic clinical definition, established by Robert Marx, the American maxillofacial surgeon who laid the foundations for the hyperbaric oxygen treatment protocol, describes ORN as exposed bone that does not heal for at least three months in the absence of residual or recurrent cancer, in a patient who has received radiotherapy. It is a simple definition, but one that hides an extremely complex biological reality.
Who is at risk of mandibular osteoradionecrosis?
Hyperbaric therapy in head and neck cancer becomes relevant especially as a preventive and therapeutic measure for post-radiotherapy complications. The patients at greatest risk are those who received irradiation for oropharyngeal cancer (cancer of the oral cavity, tonsils, or base of the tongue), laryngeal cancer, or salivary gland cancer. They receive high doses of irradiation directly in anatomical areas adjacent to the mandible, and the small blood vessels in the bone are among the first victims of radiation. Studies indicate that the incidence of ORN in head and neck cancers ranges between 2% and 22%, depending on the radiation dose, the technique used, and individual patient factors. With modern conformal irradiation and IMRT (Intensity Modulated Radiation Therapy) techniques, the incidence has fallen below 6%, but the absolute number of affected patients remains significant, given the increased survival rates in head and neck cancer.
A study published in 2019 in Radiotherapy and Oncology, based on a cohort of 1,224 patients with head and neck cancer treated with IMRT, found a 4.6% incidence of mandibular ORN, with a median interval of onset of 10.8 months after completion of radiotherapy. Translated into concrete terms: almost one in 20 patients will develop this complication in the first year after treatment.
Other important risk factors include:
- Dental extractions performed after radiotherapy represent one of the most frequent triggers. Surgical trauma from a simple extraction can open an entry point for bone necrosis in an irradiated patient.
- Smoking, poor nutrition, alcohol consumption, and poor oral hygiene significantly worsen the situation, further compromising the already reduced healing capacity of irradiated tissues.
- Diabetes mellitus is added to the list of risk factors by compromising the already existing microcirculation, a mechanism that overlaps with and amplifies the destructive effects of radiation on the small vessels in the bone.
The total radiation dose is an essential predictor of risk: a dose below 60 Gy rarely produces osteoradionecrosis (incidence of approximately 1.8%), while doses above 70 Gy increase the risk to 9%.
Symptoms of mandibular osteoradionecrosis and warning signs
Osteoradionecrosis does not appear suddenly, like a fracture or an acute infection. It insinuates itself gradually, often initially confused with a simple postoperative complication or an ordinary dental infection. This is exactly why early recognition of symptoms is essential.
The first sign the patient may notice is persistent pain in the mandible, which does not yield to usual pain medication and has no obvious dental cause. This pain is often dull, deep, and may radiate toward the ear or throat. It does not disappear after a few days; on the contrary, it tends to intensify over time.
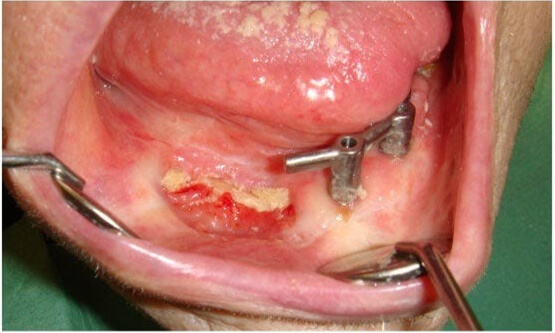
This is often followed by bone exposure in the oral cavity, in the area where the gum or oral mucosa thins and gives way, leaving visible a whitish fragment of bone without mucosal coverage. This is one of the clearest clinical indications of ORN. The exposed bone lacks blood supply, is vulnerable to infection, and does not become covered spontaneously. Patients often describe the sensation of a sharp fragment in the mouth that does not go away.
To these are added difficulties with chewing, speaking, and swallowing, symptoms that profoundly affect quality of life. Trismus (blocked mouth opening caused by muscle contracture and radiation-induced fibrosis) severely limits mandibular mobility and also makes clinical evaluation difficult.
Recurrent infections are another sign that should raise a red flag. Necrotic bone becomes an excellent substrate for bacteria. Patients may present extraoral fistulas (abnormal openings on the skin of the face or neck through which pus drains) or infections of the floor of the mouth that recur despite antibiotic treatment. Sometimes a persistent fetid halitosis also appears, impossible to control through standard oral hygiene, because of active tissue necrosis.
In advanced stages, ORN can cause pathological fractures of the mandible. We are talking about fractures that appear without major trauma, simply because the bone no longer has the mechanical resistance needed for daily life. This is a sign that the disease has progressed significantly and that therapeutic options are more limited and more complex.
Why does the bone no longer heal by itself after radiotherapy?
This is perhaps the most important question for understanding why hyperbaric therapy makes sense in the treatment of ORN. The short answer is: because radiotherapy has destroyed the biological infrastructure required for healing. The long answer requires a small detour through physiology.
The human body has a remarkable self-healing system. When a bone fractures or becomes inflamed, the surrounding cells trigger a complex repair process. Existing blood vessels dilate, new capillaries are formed within a few days, stem cells are recruited from the circulation, osteoblasts (the cells that build bone) become active and begin depositing new bone matrix. Everything works in the presence of one element fundamental to life: oxygen.
Ionizing radiation used in cancer treatment is extremely effective at destroying tumor cells, but it is not selective. It also strikes the surrounding structures, including the microvasculature, meaning the small blood vessels of the bone. The effect is not immediately visible, but it is permanent and progressive. In the months and years following radiotherapy, these vessels become fibrotic, are destroyed, and disappear. The result is a chronically hypoxic bone, with an oxygen concentration far below normal, insufficient to support regeneration processes.
Robert Marx described the mechanism in detail in 1983, defining ORN as a consequence of radiation-induced tissue hypoxia, hypovascularity, and hypocellularity. More recently, in 2004, Delanian and Lefaix completed the model by proposing the fibro-atrophic theory: radiation activates abnormal fibroblasts that produce progressive tissue fibrosis, further aggravating the deprivation of oxygen and nutrients in the bone.
Concretely, what happens in the bone? Osteoblasts, the cells responsible for bone construction, become practically nonfunctional under conditions of severe hypoxia. They require a minimum oxygen concentration to synthesize collagen and mineralize the bone matrix. Without sufficient oxygen, they do not work. Osteoclasts, the cells that break down old bone, continue to function, but the reconstruction process no longer keeps pace. The balance between degradation and reconstruction breaks, in favor of degradation.
To this is added the fact that the local immune system is also compromised: macrophages and neutrophils that should fight bacteria and clear fragments of dead tissue also need oxygen to function efficiently. A landmark study published in PubMed described as early as 1975 that hyperbaric oxygen therapy brought significant improvement in 14 patients with mandibular osteonecrosis considered intractable by other methods, precisely because it reoxygenated these tissues. The biological mechanism is simple. If you reintroduce oxygen into the equation, the healing systems can restart.
This is, in essence, the logical and biological bridge toward hyperbaric therapy.

How does hyperbaric therapy (HBOT) help in mandibular osteoradionecrosis?
Hyperbaric oxygen therapy (HBOT) is not a magical treatment and no serious clinic presents it as such. It is a treatment with well-documented biological mechanisms, acting directly on the fundamental causes of ORN. Here is how.
In a hyperbaric chamber, the patient breathes pure oxygen (100%) at an atmospheric pressure 2–3 times higher than normal. At Hyperbarium Clinic, this is performed in the Haux Starmed 2200 XL medical chamber, at a pressure of up to 3 ATA. Under these conditions, oxygen is no longer transported exclusively by hemoglobin in red blood cells; it dissolves directly into the blood plasma, reaching concentrations 10 to 20 times higher than under normal conditions. This exceptional saturation allows it to penetrate tissues with compromised microcirculation, where red blood cells can no longer physically arrive because of vascular fibrosis.
The first and most important effect is the reversal of tissue hypoxia in the affected mandibular area. Researchers have documented that, after an HBOT protocol, the partial pressure of oxygen (pO₂) in irradiated tissues increases from almost anoxic levels (below 5 mmHg) to almost normal values (above 30 mmHg), sufficient to reactivate cellular healing processes.
The second major effect is stimulation of angiogenesis, meaning the formation of new blood vessels. Hyperbaric oxygen activates the release of vascular growth factors, especially VEGF (Vascular Endothelial Growth Factor), and mobilizes endothelial progenitor cells from the bone marrow. In practice, hyperbaric therapy “tells” the body to rebuild the vascular infrastructure destroyed by radiation. A study published in PMC (PubMed Central) in 2020 documents that the healing rate of mandibular osteoradionecrosis in patients treated with hyperbaric oxygen approaches 94%. This is a remarkable result for a condition otherwise extremely difficult to treat.
The third effect is reactivation of osteoblasts. Once the tissue oxygen level returns to functional parameters, bone-building cells resume their activity. Collagen synthesis and bone mineralization restart. Combined with surgery, which removes dead necrotic tissue, HBOT creates the conditions for real bone healing.
Last but not least, HBOT has a direct antimicrobial effect. Increased oxygen concentrations are toxic to anaerobic bacteria (those that live in the absence of oxygen and frequently colonize necrotic bone) and potentiate the effect of systemic antibiotics. This explains why patients with recurrent infectious ORN respond better to antibiotic therapy when HBOT is added to the treatment scheme.
The official recognition of HBOT for this indication is explicit and strong. The European Committee for Hyperbaric Medicine (ECHM), in the 2017 consensus document, recommends HBOT in the treatment of mandibular osteoradionecrosis with a Type 1 recommendation and level B evidence, which means that the benefit is confirmed by serious clinical studies and that its use is recommended as a standard of practice. This places mandibular ORN among the first-line indications of hyperbaric therapy, alongside carbon monoxide poisoning.
A systematic review published in 2024 showed that adjuvant hyperbaric therapy brings real benefits to the quality of life of patients with ORN, reducing pain and improving xerostomia and dysphagia, even if its effect on bone healing remains under study.
The hyperbaric therapy protocol in osteoradionecrosis
Hyperbaric therapy in ORN is not applied by guesswork. There is a well-defined protocol, developed primarily by surgeon Robert Marx, which has become the global reference in the field and formed the basis of ECHM guidelines. Understanding this protocol is important both for patients and for the physicians who monitor them.
Pre-operative stage: preparing the bone for surgery with hyperbaric oxygen therapy
Before any surgical intervention on the mandible, whether it is a simple dental extraction, debridement (cleaning of necrotic bone), or a more extensive resection, patients with ORN or at high risk of ORN are recommended to undergo 20 to 30 HBOT sessions. The purpose of this stage is not complete healing, but the creation of a better oxygenated tissue environment in which surgery has a much greater chance of success. Better vascularized bone heals more easily, and the risk of wound dehiscence or extension of postoperative necrosis is significantly reduced.
The classic Marx protocol, described in detail in a PMC article and confirmed by multiple clinical studies, provides for 30 preoperative HBOT sessions at a pressure of 2.4 ATA, with 100% oxygen, for 90 minutes per session, five days per week. At Hyperbarium Clinic, each session lasts on average 120 minutes, at a pressure that can reach 3 ATA, which aligns with international protocols and may offer, in certain cases, superior tissue penetration.
If after the 30 sessions a significant improvement is observed (the mucosa becomes covered, pain decreases, there are no longer signs of active infection), the patient may continue up to a total of 60 sessions, without the need for major surgery. Resolution of ORN through HBOT alone or with debridement is the favorable situation of stage I of Marx’s protocol.
Post-operative stage: how many hyperbaric therapy sessions are needed
If surgery is nevertheless necessary, either to remove fragments of dead bone or for mandibular resection with subsequent reconstruction, hyperbaric oxygen therapy continues after the operation as well. Usually, 10 additional postoperative sessions are performed to support healing of the surgical wound and prevent infectious complications.
The reference 20/10 protocol means 20 preoperative sessions followed by 10 postoperative sessions. This scheme is most often used in the prevention of ORN in patients who require dental extractions in irradiated areas. Long-term results are significantly better than surgery without HBOT. A prospective observational study that followed 411 patients over 8 years documents that 92% of patients in the group treated with the above-mentioned protocol achieved complete healing.

Total number of sessions and monitoring
The total number of HBOT sessions in mandibular osteoradionecrosis usually varies between 30 and 40 sessions for moderate cases and can reach 60 for complex cases or recovery after mandibular resection. There is no universal fixed number. The protocol is adapted individually, depending on the stage of the disease, the clinical response, the type of associated surgical intervention, and the patient’s general condition.
At Hyperbarium Clinic, every patient with osteoradionecrosis benefits from a personalized treatment plan, established before the first session during the initial medical consultation. The hyperbaric physician evaluates the oncological history, the total radiation dose received, the current stage of ORN, and possible comorbidities, and only after this complete evaluation establishes the number of sessions, working pressure, and any recommended adjuvant therapies. The plan is not rigid: it is reviewed periodically throughout the treatment, according to the clinical evolution of each patient.
During treatment, periodic clinical monitoring is essential. The physician evaluates the evolution of the mucosa, the degree of scarring, the absence of signs of infection, and, where appropriate, radiological or computed tomography images to verify bone changes. This careful monitoring allows the protocol to be adjusted in real time. One additional session or a modification of pressure parameters can make the difference between complete healing and relapse.
The Hyperbarium team also provides support and guidance throughout treatment, from step-by-step explanation of the procedure before the first session (to remove anxiety related to the enclosed space of the hyperbaric chamber), to basic nutritional counseling and oral hygiene recommendations adapted to the patient’s condition. Patients are encouraged to report any new symptom that appears between sessions, and the medical team is available for additional consultations whenever the clinical situation requires it.
An important element to emphasize is that hyperbaric therapy is well tolerated by the vast majority of patients. Adverse effects, such as a feeling of pressure in the ears (which improves through simple equalization maneuvers, similar to those used on an airplane), mild fatigue, and, extremely rarely, temporary myopia, are minor and transient. The risk of barotrauma or oxygen toxicity is negligible under correct medical protocols and professional monitoring provided within the clinic.

Prevention of mandibular osteoradionecrosis: how can this complication be avoided?
Prevention and early treatment of mandibular osteoradionecrosis have become more accessible with advances in irradiation techniques. Thus, the rate of mandibular osteoradionecrosis has decreased considerably compared with previous decades. Nevertheless, prevention remains the central pillar of managing this condition. And hyperbaric therapy plays an important role in prevention as well, not only in treatment.
Any patient who is undergoing or has undergone radiotherapy in the head and neck area and subsequently requires dental extractions or other oral surgical interventions should be evaluated by a specialist in hyperbaric medicine before the procedure. Administering a preoperative hyperbaric oxygen therapy protocol in these situations dramatically reduces the risk of triggering post-extraction ORN. And this is one of the most frequent entry points of the disease.
Pre-radiotherapy dental consultation is also of maximum importance: extracting compromised teeth before irradiation begins is much safer than extraction after irradiation. Also in the pre-radiotherapy stage, meticulous oral hygiene, preventive fluoridation, and patient education regarding risks contribute significantly to reducing the incidence of ORN.
Why does access to a specialized hyperbaric medical center matter?
All the benefits of HBOT described in this article critically depend on one essential condition: treatment must be administered in a certified medical chamber, at correct parameters (minimum pressure of 2.4–3 ATA, 100% oxygen), by a medical team experienced in hyperbaric medicine. Not all hyperbaric chambers available on the market meet these standards.
mHBOT hyperbaric chambers (mild hyperbaric oxygen therapy), often available in spas or as personal-use devices, do not reach the pressure parameters needed to treat osteoradionecrosis or other certified medical indications. At a pressure of 1.3–1.5 ATA, the concentration of oxygen dissolved in plasma is entirely insufficient to produce the angiogenesis or osteoblast reactivation documented in studies. There are no clinical studies validating their efficacy in ORN or in other first-line medical indications.
Hyperbarium Clinic in Oradea has the Haux Starmed 2200 XL chamber, a certified Class IIB medical device with safety class A, with 16 seats, operating at pressures of up to 3 ATA. The medical team is led by Dr. Ciprian Sturz, with over 15 years of experience gained in university clinics in Germany such as Klinikum Nürnberg and Klinikum Roth. The protocol applied to patients with osteoradionecrosis follows ECHM recommendations and is integrated with maxillofacial surgery and oncology teams for complete case management.
Mandibular osteoradionecrosis is a serious condition, but not one without hope of treatment. The earlier it is diagnosed, the faster access to hyperbaric therapy is obtained, and the more coordinated the medical team is, the greater the chances of healing. Hyperbaric therapy does not eliminate the need for surgical treatment in advanced cases, but it makes it possible where otherwise it would not be and, many times, makes it unnecessary simply by restoring to the bone the capacity that radiation had stolen from it: the ability to heal itself.

